Medicaid-approved NEMT provider.
NPI # 1407551989
NPI # 1407551989
Getting discharged from the hospital sounds simple until you stop and think about what happens next. How will the patient get home? Can they sit in a regular car? Will someone be there to help once they arrive? Those questions can turn a good moment into a stressful one fast.
The ride home is not just a ride. It is part of the discharge plan. Think of it like a bridge between hospital care and home recovery. If that bridge feels shaky, the whole transition feels harder. That is why early planning matters so much. Official discharge guidance and discharge-planning research point in the same direction: patients do better when the plan is clear, support is in place, and the next steps are not left until the last minute [1][4][5].
A lot of families wait until the hospital says, “You can go home now.” That is understandable, but it often creates unnecessary stress. MedlinePlus says the discharge plan should be created before the patient leaves the hospital, and the care team should work on that plan with the patient and family or friends [1].
Key point: Transportation should be treated like part of medical discharge planning, not like a last-minute errand.
That matters because the patient may need more than a ride. They may need help with transfers, a wheelchair, oxygen, or someone waiting at home. A 2018 study found that support at home was one of the predictors of discharge readiness, and lower readiness for discharge was linked with a higher risk of unplanned readmission and death within 30 days [5].
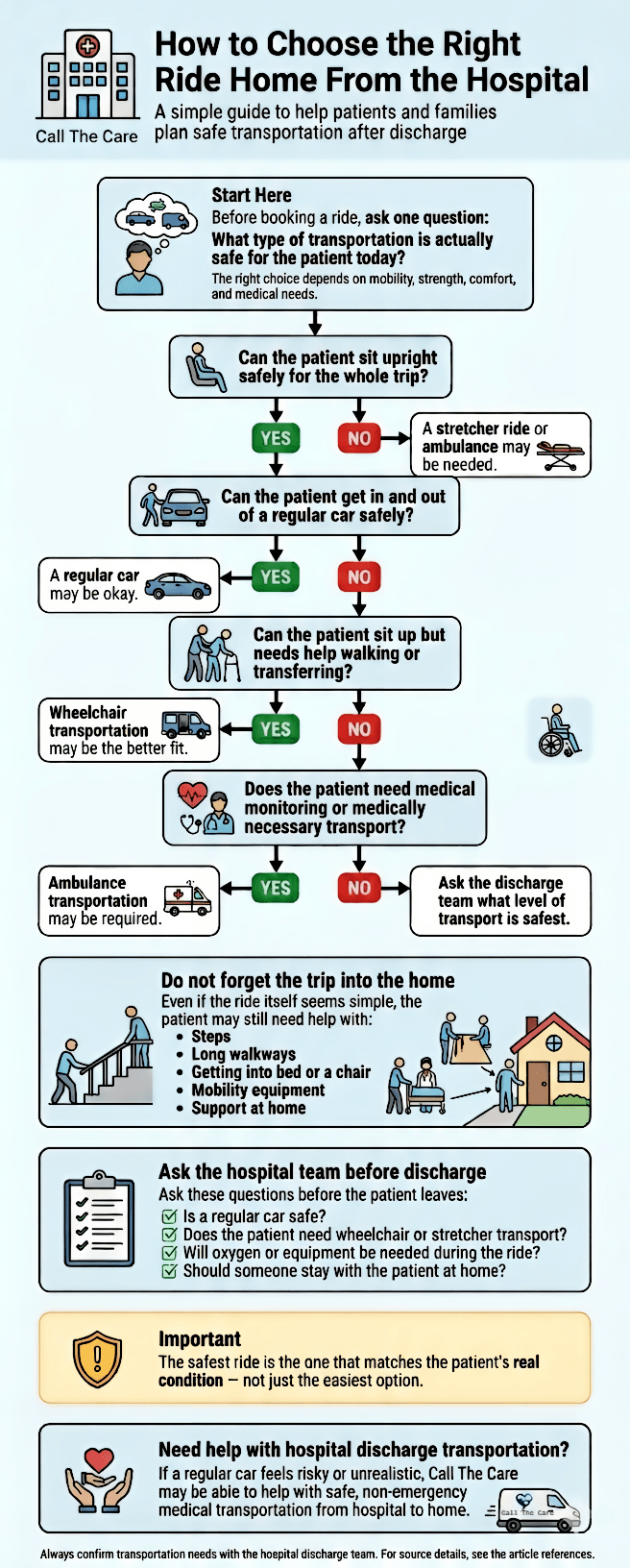
Before anyone books transportation, start with one basic question: What is actually safe for this patient today?
A person who walked into the hospital on their own may not be able to get into a regular car safely after surgery, illness, weakness, dizziness, or heavy pain medication. That is why it is worth asking a few direct questions before discharge [1][4].
Ask the care team these questions before discharge:
These are not small details. Social-support research found that after discharge, patients often need practical help with daily care, medical care, and transportation. Patients who lacked enough support after discharge had a higher risk of readmission [6].
A regular car may work when the patient can sit upright safely, tolerate the ride, and get in and out without major difficulty. In those cases, a family pickup may be perfectly reasonable.
Wheelchair transportation may be the better fit when the patient can sit up but cannot walk far, has people with mobility challenges, feels weak, has major balance issues, or needs more support from pickup to drop-off. This option can make discharge easier when a regular car feels like too much of a struggle.
Stretcher or ambulance transportation may be needed when the patient cannot sit upright safely or when using another vehicle could put their health at risk. Medicare says Part B covers ground ambulance transportation when traveling in any other vehicle could endanger the patient’s health. In some non-emergency cases, Medicare may pay when there is a written order showing the transport is medically necessary [2].
Key point: Do not guess. Ask the nurse, doctor, or discharge planner what kind of ride is medically safe.
Not sure which option fits your situation?Here’s a simple visual guide to help you decide quickly.
Now let’s look at what needs to be ready once the patient gets home.
Getting home is only half the job. The patient also has to get into the home, settle in safely, and manage the first few hours and days.
This is where many families get caught off guard. The ride goes fine, but then the patient gets home and there is no walker, no shower chair, no clear path to the bed, and no one available to help. It is a bit like bringing home a fragile package and realizing there is nowhere safe to put it.
MedlinePlus says patients and caregivers should plan ahead for arrival home and ask whether equipment or supplies will be needed, such as a wheelchair, walker, cane, shower chair, portable toilet, or oxygen [1]. AHRQ’s RED Toolkit also highlights organizing post-discharge equipment, at-home services, medicines, and written discharge instructions the patient can understand [4].
Before the patient arrives home, try to have these basics covered:
Families often feel like they have to solve everything themselves. Usually, they do not.
Depending on the hospital, the discharge plan may involve the doctor, the nurse, a case manager or discharge planner, the family caregiver, and the transportation provider. Research on hospital-to-home transitions found that patients and caregivers do better when they are included in planning, rather than being handed instructions at the very end [1][7].
Key point: If you are the caregiver, your role matters. Speak up early and ask what the patient will need during the trip and after arrival.
You do not need medical training to ask good questions. You just need to keep them clear.
Ask these before discharge:
What kind of ride is safe? Ask whether a regular car is appropriate or whether wheelchair, stretcher, or ambulance transportation is safer.
What can the patient safely do today? Discharge instructions should explain activity limits, including whether the patient can walk safely, use stairs, or carry anything [1].
What equipment should be ready at home? That may include a walker, wheelchair, oxygen, bedside commode, or shower chair [1][4].
Will the patient need help at home during the first 24 to 48 hours? Support at home can make a real difference in how ready a patient is for discharge and how safely they recover [5][6].
What follow-up care is already scheduled? A strong discharge plan should cover more than the ride home. It should also cover what happens next [1][4].
Who should we call if something goes wrong? The discharge plan should clearly tell the patient and caregiver who to contact with questions or urgent concerns [1].
Families often try to handle everything themselves. Sometimes that works well. Sometimes it adds stress at exactly the wrong time.
If the patient has trouble walking, cannot safely transfer into a car, needs more hands-on help from pickup to drop-off, or the family is not sure what is safest, professional non-emergency medical transportation may be the better option. The goal is not to make things fancy. It is to make the trip safer and less stressful.
That does not mean every hospital discharge needs a specialty ride. It simply means the ride should match the patient’s condition. In situations like these, a provider such as Call The Care can be a practical option when a regular car feels risky or unrealistic.
Key point: The safest discharge ride is the one that fits the patient’s real needs, not just the easiest option on paper.
Need help arranging the ride home? Schedule hospital discharge transportation with Call The Care.
One of the biggest mistakes families make is focusing only on discharge day. The better question is: What will the next seven days look like?
AHRQ’s RED Toolkit puts a lot of weight on the post-discharge side of the process, including follow-up care, equipment, medicines, and patient understanding of the plan [4]. Research also suggests that better discharge support and stronger discharge teaching can improve the transition home and reduce unplanned readmissions in some patient groups [7][8].
That first week may include:
Medicaid guidance also notes that transportation is a required part of access to covered care in Medicaid, and CMS describes necessary transportation as a service with a direct impact on health outcomes [3].
Waiting until discharge day to arrange the ride.
This usually makes the whole process harder than it needs to be.
Assuming a family car is always safe.
It may not be, especially after surgery, a fall, or a long hospital stay.
Forgetting about stairs, long walkways, or apartment access.
The patient may handle the ride but still struggle to get into the home.
Not having equipment ready.
A safe trip home often depends on what is already waiting there [1][4].
Ignoring follow-up transportation.
The ride home is only the first step in recovery [3][4].
Planning transportation from hospital to home is not just about getting from Point A to Point B. It is about making sure the patient can leave safely, arrive safely, and recover with the right support already in place.
The best plan starts early, fits the patient’s actual condition, and covers more than the ride itself. Can the patient sit up? Can they transfer safely? Is the home ready? Is someone there to help? When those questions are answered before discharge, the whole process gets smoother.
That is the real goal. Not just getting home, but getting home well [1][4][5].
1. Can a patient go home from the hospital in a regular car? Yes, sometimes. A regular car may work if the patient can sit upright, tolerate the ride, and get in and out safely. The hospital team should confirm whether that is a safe option [1].
2. When should a family choose wheelchair transportation instead of a car? Wheelchair transportation may make more sense when the patient can sit upright but cannot walk far, has major weakness, or needs more support during pickup and drop-off.
3. Does Medicare pay for transportation from hospital to home? Medicare may cover medically necessary ambulance transportation when another vehicle could endanger the patient’s health. It does not automatically cover every type of ride home [2].
4. What should be ready at home before discharge? The patient may need mobility equipment, medicines, basic supplies, and someone to help during the first hours or days at home. The discharge team should explain what is needed [1][4].
5. Why should follow-up transportation be planned before discharge? Because recovery does not end at the front door. Follow-up visits, therapy, and other care often start soon after discharge, and transportation is part of making that care possible [3][4].
[1] MedlinePlus. Leaving the hospital - your discharge plan. U.S. National Library of Medicine. https://medlineplus.gov/ency/patientinstructions/000867.htm
[2] Medicare.gov. Ambulance services. https://www.medicare.gov/coverage/ambulance-services
[3] Medicaid.gov. Assurance of Transportation. https://www.medicaid.gov/medicaid/benefits/assurance-of-transportation
[4] Agency for Healthcare Research and Quality. Re-Engineered Discharge (RED) Toolkit. https://www.ahrq.gov/patient-safety/settings/hospital/red/toolkit/index.html
[5] Kaya S, Guven GS, Aydan S, et al. Patients' readiness for discharge: Predictors and effects on unplanned readmissions, emergency department visits and death. Journal of Nursing Management. 2018. https://pubmed.ncbi.nlm.nih.gov/29573007/
[6] Schultz BE, Corbett CF, Hughes RG, Bell N. Scoping review: Social support impacts hospital readmission rates. Journal of Clinical Nursing. 2022. https://pubmed.ncbi.nlm.nih.gov/34866259/
[7] Chen L, Xiao LD, Chamberlain D, Newman P. Enablers and barriers in hospital-to-home transitional care for stroke survivors and caregivers: A systematic review. Journal of Clinical Nursing. 2021. https://pubmed.ncbi.nlm.nih.gov/33872424/
[8] Lin L, Fang Y, Wei Y, et al. The effects of a nurse-led discharge planning on the health outcomes of colorectal cancer patients with stomas: A randomized controlled trial. International Journal of Nursing Studies. 2024. https://pubmed.ncbi.nlm.nih.gov/38676992/




